Benign lump
Much of the surgery required to remove benign lumps is straightforward. It involves finding a natural plane between the lump and surrounding healthy, natural hard or soft tissue. This can only be learned by feel. Most of surgery is “doing” not “talking”. We have therefore only given a brief description that may be relevant to patients, carers or neophyte surgeons.
Benign lumps of the mouth, jaws and face
Brown tumour of hyperparathyroidism
After diagnosis by incisional biopsy, treatment is by local excision and curettage (scraping) of bone and periosteum (dense connective tissue enveloping bones) - if the lesion does not regress spontaneously after treatment of the underlying hyperparathyroidism.
Congenital (present at birth) epulis
Treatment by local excision in a subperiosteal (beneath the periosteum) plane is curative.
Epulis
After classification from clinical examination and/or imaging features, management of these lesions is according to the diagnosis. Most are simply excised in the described “natural plane”.
Fibroepithelial polyp
These lesions once diagnosed either on a clinical basis or by incisional biopsy, should be excised including their base. The pedunculated lesion often has a very vascular stalk which will require local control with diathermy (stopping bleeding by use of electrical heating device) or sutures.
Granuloma
Local granulomata are usually treated by simple local excision. In the case of orofacial granulomatosis and sarcoidosis, intralesional application of steroids may help. In the case of orofacial granulomatosis, patch testing for allergic-type responses to cinnamates (often found in toothpastes) should be undertaken. Elimination diets, to exclude dietary causes, can be both diagnostic and therapeutic and may prevent serious later facial distortion (see Figure 1).

Giant cell granuloma (giant cell epulis)
Treatment is by excision that should include the underlying periosteum.
Gingival fibromatosis
Treatment is excision by gingivectomy, unless the drugs can be changed and this change induces an involution of the swelling.
Haemangioma
It should be remembered that 80% will resolve spontaneously. Some will respond to the use of steroids or propanolol to promote resolution. Localised cryotherapy (freezing) and laser therapy can also resolve these lesions.
Hyperplasia
Treatment consists of removing the offending denture to see if there is any spontaneous resolution. If there is, then it may be possible to manage this non-surgically. If there is no such spontaneous resolution, the area should be excised, allowed to heal and then new dentures provided. Simple pre-prosthetic measures may also be needed to prevent future similar problems.
Lipoma
Treatment consists of excision with primary repair.
Papilloma
Treatment is by excision biopsy.
Pyogenic granuloma
Treatment is excision, usually in a deep plane, if the lesion causes symptoms.
Vascular malformations
Treatment is conventionally by interventional radiology; either embolization or sclerosant (a range of chemicals are being used for this purpose) injection, coupled with surgical excision and reconstruction where indicated. As the move towards minimal intervention by embolization techniques has progressed, it is important to recognise that these malformations tend to recur without synchronized excision.
Benign lumps of the neck
Cervical lymphadenopathy (enlargement of lymph nodes in the neck)
For the treatment of atypical mycobacterial lymphadenitis, there is a balance needed between surgical treatment (which remains the most effective modality) and watching and waiting with long-term clarithromycin treatment (clarithromycin is a macrolide antibiotic drug, used for the treatment of a range of bacterial infections of the skin and respiratory tract). Clarithromycin treatment may avoid an operation but can take a very long time and sometimes leaves scars worse than those of surgery.
Sternomastoid tumour
Treatment is direct physiotherapy and manipulation if possible. If this condition has been missed as a child and presents in later life, formal excision (cranial and caudal ends of the sternomastoid muscle, with or without Z-plasty (Z-shaped incision)) may be necessary because areas of extremely tight fibrosis and sometimes ossification can occur.
Neurofibroma
Isolated neurofibromas can be excised although usually the nerve will be irrevocably damaged by the excision and will require primary nerve repair.
Schwannoma
Schwannomas can often be excised while maintaining the integrity of the nerve of origin.
Paraganglioma
These tumours should be excised because they are at the risk of spreading into the cranial cavity. These are extremely vascular tumours and as most of them are crossed by the internal carotid artery, there is a high level of risk of vascular injury
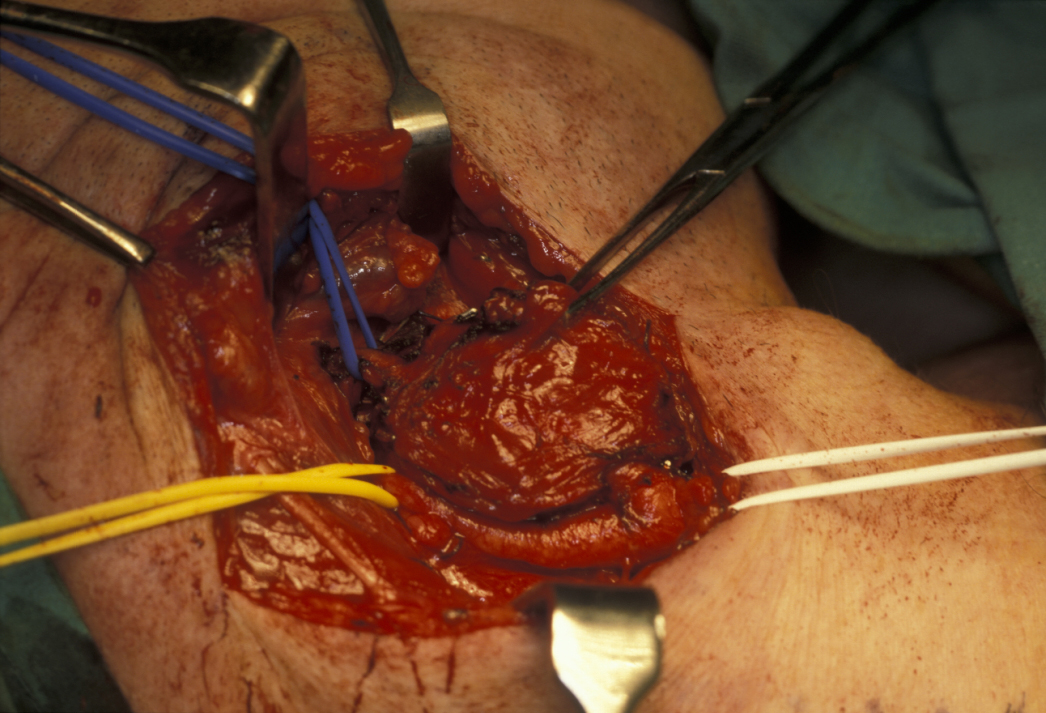
Carotid body tumours
Not all carotid body tumours should be removed because most of these are benign. However, young healthy patients benefit from excision (see Figure 2). Patients who are having symptoms but are at high risk for surgery may respond to localised radiotherapy.
Pharyngeal pouch
There are a range of endoscopic and open treatment procedures for the excision of pharyngeal pouches. The profusion of different treatments would suggest that no one is ideal but most are nowadays managed endoscopically.