Fistula
There are four paired cavities (sinuses), essentially extensions to the nose. Of these paranasal sinuses the maxillary sinus (also known as the antrum) is of greatest significance in the context of oral and maxillofacial surgery. This cavity is located right above the upper jaw, with only a thin layer of bony separation and in direct contact with the teeth in the upper jaw. This is of general relevance with regard to diagnosis of conditions that may arise in the mouth and appear to manifest in the maxillary sinus – or the other way around.
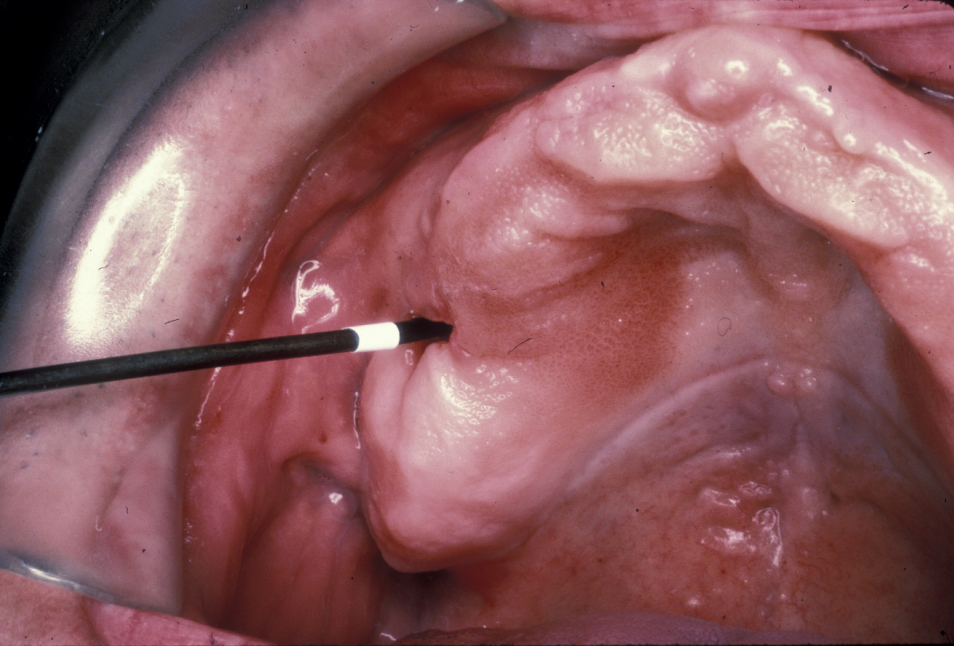
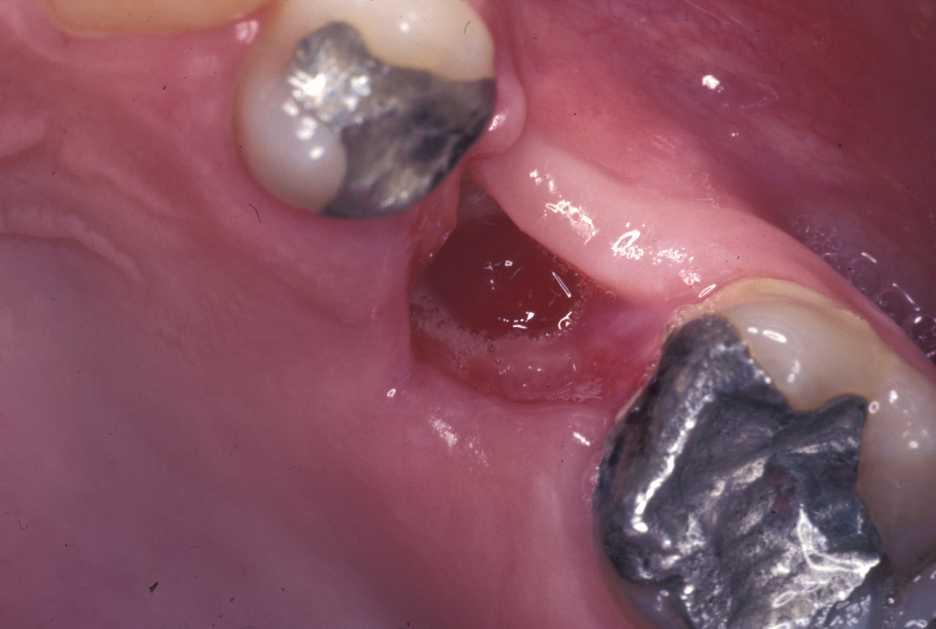
An oroantral fistula (a communication between the oral cavity and the maxillary sinus (antrum) is a common condition. Lining of the antrum may prolapse through such a fistula (Figure 1), or the fistula will have become lined with epithelium (thin, surface-covering tissue) as shown in Figure 2.
A fistula differs from a sinus in being an epithelial lined connection between a cavity to another cavity or the outside or inside body surface. A sinus may be epithelium lined but originates from an abscess, retained tooth root or area of necrotic bone. A fistula connecting the mouth and maxillary antrum starts as a communication before it becomes lined with epithelium. This is important to understand when it comes to treatment of the fistula.

The most common cause of an oroantral fistula is the extraction of a single standing molar tooth with multiple roots, especially with hypercementosis (excessive formation of mineralised tissue around the root of a tooth) present. If such a tooth root is in close proximity to the antrum, chances are high that extraction of the tooth may lead to the formation of an oroantral fistula.
An established (chronic) oroantral fistula (Figure 3) leads to bouts of recurrent maxillary sinusitis, there may be a foul taste in the mouth, and fluids may be passing from the mouth through the fistula and out of the nose. The fistula can be demonstrated by occluding the nose and blowing out through the nose: air will be seen to bubble out of the fistula. A plain X-ray radiograph helps to identify any fragments of retained roots in the sinus.